
 ภาพด้านบน: รูป A เป็น CT ที่แสดงให้เห็น lytic lesion ที่ head of left clavicle ซึ่งเป็น single site of bone metastasis และผู้ป่วยมีอาการปวด. รูป B แสดงให้เห็น cryoablation probes อยู่ภายใน lesion ขณะให้การรักษาด้วย cryoablation. ภาพจาก Callstrom, et al. Skeletal Radiology (Jan 2006)
ภาพด้านบน: รูป A เป็น CT ที่แสดงให้เห็น lytic lesion ที่ head of left clavicle ซึ่งเป็น single site of bone metastasis และผู้ป่วยมีอาการปวด. รูป B แสดงให้เห็น cryoablation probes อยู่ภายใน lesion ขณะให้การรักษาด้วย cryoablation. ภาพจาก Callstrom, et al. Skeletal Radiology (Jan 2006)
เมื่อสัปดาห์ก่อนที่ MGH Radiology, มีงานมอบรางวัลให้กับ researcher ทางด้าน Musculoskeletal imaging ที่สร้างสรรค์ผลงานที่มีประโยชน์กับวงการแพทย์ เป็นรางวัลที่มอบให้กับ Dr.Callstrom จาก Mayo Clinic Radiology มีเนื้อหาเกี่ยวกับการพัฒนาเทคนิก image-guided ablation ในการให้ palliative treatment ของ bone metastasis ก็เลยเก็บข้อมูลมาฝากกันครับ
Pain Palliation of Bone Metastasis: Significance
- ประมาณ 40% ของผู้ป่วยที่เป็น cancer มี bone metastasis
- ประมาณครึ่งหนึ่งของผู้ป่วยที่มี metastatic cancer ทนทรมานกับอาการปวดที่ uncontrolled ด้วยการรักษาแบบ conventional (เช่่น ยา, การฉายแสง) และได้รับผลข้างเคียงจากการรักษาดังกล่าว
Conventional Treatments for Painful Bone Metastasis
- Pain medication มีข้อด้อยที่ผลข้างเคียงของยา
- Radiation therapy พบว่าอัตราการตอบสนองยังไม่สูุงมาก ผู้ป่วยประมาณ 20% - 40% ไม่ตอบสนองต่อการรักษา (ยังปวดอยู่) และ median duration of response แค่ 2-4 เดือน
- Surgical therapy เช่นการใส่ prosthesis
Percutaneous Ablation of Painful Bone Metastasis
- Option ใหม่ในการรักษา painful bone metastasis ที่ปัจจุบันอยู่ใน clinical trial
- ให้การรักษากับ painful bone metastasis ที่ limited อยู่ที่ 1-2 ตำแหน่ง, มี CT correlation กับอาการของผู้ป่วย (เห็น lesion ใน CT), อยู่ในตำแหน่งที่เข้าถึงได้โดย percutaneous technique และเป็น lytic or mixed bone metastasis
- ข้อห้ามในการทำ คือ acute spinal cord compression, diffuse disease, และ radicular symptoms
- Cryoablation preferred over Radiofrequency ablation เนื่องจากสามารถ monitor การเปลี่ยนแปลงที่เกิดขณะทำการรักษาได้ และอาการปวดระหว่างการรักษาน้อยกว่า
- ทำการรักษา under general anesthesia, CT or ultrasound guidance โดยเฉลี่ยใช้เวลาประมาณ 2 ชั่วโมง
Reference: Callstrom, et al. Painful Metastases Involving Bone: Percutaneous Image-guided Cryoablation—Prospective Trial Interim Analysis. Radiology 2006; 241: 572.
April 30, 2008
Palliative Treatment for Painful Bone Metastasis with Percutaneous Ablation
April 28, 2008
When to Perform Breast MRI?
 ภาพด้านบน: MRI of both breasts (with gadolinium, subtraction image) แสดงให้เห็น irregular enhancing mass in the left breast ผล biopsy พบว่าเป็น invasive ductal carcinoma (สังเกตว่า เวลาอ่าน breast MRI, right breast จะอยู่ด้านซ้ายของภาพ และ left breast อยู่ด้านขวาของภาพเนื่องจากผู้ป่วยนอนคว่ำขณะทำการตรวจ)
ภาพด้านบน: MRI of both breasts (with gadolinium, subtraction image) แสดงให้เห็น irregular enhancing mass in the left breast ผล biopsy พบว่าเป็น invasive ductal carcinoma (สังเกตว่า เวลาอ่าน breast MRI, right breast จะอยู่ด้านซ้ายของภาพ และ left breast อยู่ด้านขวาของภาพเนื่องจากผู้ป่วยนอนคว่ำขณะทำการตรวจ)
คงเป็นที่ทราบกันดีนะครับว่าการทำ breast cancer screening ในปัจจุบันได้รวมการตรวจทางรังสีวิทยาด้วยการทำ mammography เข้าไว้ด้วย และถือเป็นองค์ประกอบที่สำคัญมาก ในการวินิจฉัย breast cancer พบว่ารังสีแพทย์มีบทบาทในการวินิจฉัย breast cancer มากขึ้นเรื่อยๆ เนื่องจากผู้ป่วยส่วนหนึ่งมาทำ mammogram และเมื่อพบความผิดปกติ รังสีแพทย์ก็ทำ biopsy เลย และในหลายๆ ครั้งก็เป็นหมอคนแรกที่ให้การวินิจฉัยแล้วจึงส่งต่อไปยังศัลยแพทย์ครับ ประโยชน์ของการทำ mammogram นั้นเป็นที่ประจักษ์อยู่ในบทความและหนังสือทั่วไปมากมายนะครับ
อย่างไรก็ตาม ทั้งการตรวจเต้านมและการทำ mammography ก็มีข้อจำกัดที่ไม่สามารถตรวจพบ cancer ได้ 100%. Sensitivity ของ clinical exam นั้นอยู่ที่ 50% ในขณะที่ mammography 68% ถ้ารวมกันจะมี sensitivity สูงขึ้นเป็น 77% ซึ่งก็ถือว่าสูงพอสมควร
ฺBreast MRI ได้เข้ามามีบทบาทมากขึ้นเรื่อยๆ เนื่องจากมี sensitivity สูงมากกว่า 90% ในการ detect breast cancer แต่ข้อด้อยอยู่ที่ specificity ที่ค่อนข้างต่ำกว่าวิธีการตรวจอื่นๆ ปัจจุบัน American Cancer Society (ACS) ก็ได้นำ breast MRI เข้ามาใน recommendation ด้วยครับ
Recommended Indication for Breast MRI Screening (as an Adjunct to Mammography)
1. >20% - 25% calculated lifetime risk of breast cancer (สามารถคำนวณได้จาก website ของ ACS แต่ข้อมูลปัจจุบันยังจำกัดอยู่กับคน Caucasian)
2. Documented BRCA mutation
3. First-degree relative with BRCA mutation
4. First-degree relative with premenopausal breast cancer
5. Radiation to chest between age 10 and 30 years
6. Li-Fraumeni, Cowden, or Bannayan-Riley-Ruvalcaba syndromes, or a first-degree relative with these syndromes
สิ่งควรรู้
- ไม่แนะนำให้ทำ annual breast screening with MRI ในบุคคลทั่วไปเนื่องจาก false positive เยอะ ทำให้อัตราการ biopsy ที่ไม่จำเป็นสูง
- อาจพิจารณาทำ MRI ในผู้หญิงที่ได้รับการวินิจฉัยว่าเป็น breast cancer ใหม่ เพื่อค้นหา additional lesion ใน breast ข้างเดียวกันและข้างตรงข้าม (พบว่าผู้ป่วยที่มี breast cancer มี second focus of cancer ใน breast ข้างเดียวกัน 10% ซึ่งอาจเปลี่ยนแนวทางการรักษาจาก lumpectomy เป็น mastectomy)
- แนะนำให้ทำ breast MRI ในกรณีที่พบว่าผู้ป่วยมีแต่ axillary nodal metastasis แต่ไม่พบ primary
Reference:
1. Miller JC, et al. When is breast magnetic resonance imaging recommended for cancer detection? J Am Coll Radiol 2008;224-226.
2. Saslow D, et al. American cancer society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007;57:75-89.
April 25, 2008
Postcatheterization Pseudoaneurysm - Thrombin Injection
คราวก่อน กล่าวถึงเรื่องการวินิจฉัย PSA ไปแล้วนะครับ ครั้งนี้ขอยืมภาพจากครั้งก่อน (ภาพแรก) มาให้ดูกันอีกทีครับ PSA มีลักษณะของ Yin-Yang sign ใน color Doppler ultrasound ดังที่เห็นครับ สิ่งสำคัญที่ต้องหาคือ neck ของ PSA ว่าแคบ กว้างแค่ไหน, ขนาดของ PSA เท่าไร เพื่อจะได้ประเมินว่าควรจะรักษาด้วย percutaneous technique หรือ open surgery
เมื่อใดควรรักษาด้วย Open Surgery?
1. PSA ขนาดใหญ่ที่ทำให้เกิด skin necrosis, compression of nerves or blood vessels
2. Neck of PSA กว้าง (เสี่ยงต่อการเกิด distal embolization เวลาทำ thrombin injection)
3. PSA จากสาเหตุอื่นๆที่ไม่ใช่ postcatheterization
ภาพที่สองแสดงให้เห็นหลังจากการฉีด Thrombin เข้าไปในตัว PSA ผ่านทาง needle. PSA completely thrombosed. สิ่งสำคัญคือต้องมั่นใจว่าเข็มอยู่ในตัว PSA ไม่ใช่ native vessel และต้องตรวจดูหลังจากทำเสร็จว่ามี flow ใน native artery and vein (โดยทั่วไปจะเห็นว่า flow ไปที่ CFA ชัดเจนมากขึ้นเนื่องจากไม่มี diversion ไปที่ PSA แล้ว) (ดังภาพที่ 3)
สิ่งสำคัญคือต้องมั่นใจว่าเข็มอยู่ในตัว PSA ไม่ใช่ native vessel และต้องตรวจดูหลังจากทำเสร็จว่ามี flow ใน native artery and vein (โดยทั่วไปจะเห็นว่า flow ไปที่ CFA ชัดเจนมากขึ้นเนื่องจากไม่มี diversion ไปที่ PSA แล้ว) (ดังภาพที่ 3) ต้องนำผู้ป่วยมาตรวจอัลตราซาวด์ซ้ำที่ 24-72 ชั่วโมงหลังเสร็จ procedure เพื่อให้มั่นใจว่า PSA thrombosed ไปหมดแล้วจริง
ต้องนำผู้ป่วยมาตรวจอัลตราซาวด์ซ้ำที่ 24-72 ชั่วโมงหลังเสร็จ procedure เพื่อให้มั่นใจว่า PSA thrombosed ไปหมดแล้วจริง
Facts: - Thrombin is not FDA-approved for intravenous injection (keep in mind). - Worst complication is distal embolization of clot - Primary success rate reported between 91% - 100%
Reference: Webber GW, et al. Circulation 2007;115:2666-2674.
ผู้เขียนขออุทิศทุกบทความเกี่ยวกับ percutaneous radiological procedures ในบล้อกนี้ที่เขียนขึ้นโดยตัวผู้เขียนเอง ให้กับ Dr. Kenneth Nazinitsky ผู้ประสิทธิ์ประสาทความรู้ ถ่ายทอดประสบการณ์ และให้โอกาสผู้เขียนในการทำ procedure ต่างๆ มากมาย ตลอดระยะเวลา 1 ปีที่ทำงานเป็น clinical fellow ที่ Ohio. Dr. Nazinitsky เสียชีวิตอย่างสงบในเดือนมีนาคม 2551.
April 22, 2008
What is Bronchioloalveolar Carcinoma (BAC)?
 Bronchioloalveolar carcinoma (BAC) เป็น subtype หนึ่งของ lung adenocarcinoma
Bronchioloalveolar carcinoma (BAC) เป็น subtype หนึ่งของ lung adenocarcinoma
อ้างอิงจาก WHO 2004, Lung Adenocarcinoma มีลักษณะทาง pathology ที่ heterogeneous มีได้หลาย subtype และสามารถพบหลาย subtype ภายใน tumor เดียว (ปัจจุบันพบว่า adenocarcinoma subtype ที่พบบ่อยที่สุด คือ mixed subtype).
ข้อแตกต่างของ BAC จาก subtype อื่นของ adenocarcinoma
1) pure lepidic growth
2) ไม่มี invasion ของ stroma, blood vessel หรือ pleura
3) Prognosis ดีมาก
จากภาพ CT ตัวอย่างจะเห็นว่ามี groundglass nodule ที่ left lower lobe ถ้าสังเกตให้ดีจะเห็นว่ามี bubbly appearance ซึ่งเป็น low attenuating areas ภายในตัว tumor
Differential Diagnosis of Solitary Groundglass Pulmonary Nodule
- Neoplasm
- Inflammation/infection
- Focal hemorrhage
- Focal interstitial fibrosis
จะเห็นว่า differential diagnosis กว้างมาก สิ่งที่จะช่วยแยกแยะว่า groundglass nodule มีสาเหตุจากอะไรคือ การดูภาพเปรียบเทียบ (ถ้ามี) และการทำ follow up CT
Differential Diagnosis of 'Persistent' Solitary Groundglass Nodule
- Neoplasm (BAC, adenocarcinoma with BAC feature, Atypical Adenomatous Hyperplasia)
- Focal interstitial fibrosis
References:
1. Park CM, et al. Radiographics 2007;27:391-408.
2. Travis WD, et al. J Clin Onc 2005;23:3279-3287.
April 20, 2008
Postcatheterization Pseudoaneurysm (1)

Incidence of Pseudoaneurysm (PSA)
after diagnostic catheterization = 0.05% - 2%
after percutaneous intervention = 2% - 6%
Natural history of PSA
1. Spontaneous thrombosis ส่วนมากก็จะหายได้เองแต่ใช้เวลาเป็นสัปดาห์ ทั้งนีี้ในผู้ป่วยที่ on anticoagulation (รวมถึง antiplatelet e.g. aspirin, clopidogrel) ก็อาจใช้เวลานานกว่านี้
2. Rupture โอกาสขึ้นกับ ขนาด PSA, อาการ, large hematoma และ growth ของ PSA
Factors Associated with PSA Formation
- ยาที่ผู้ป่วยได้รับ (antiplatelet, anticoagulation)
- Procedure (ใช้ sheath ขนาดใหญ่, ทำทั้ง vein/artery, ทำ intervention ด้วย, กดไม่ดีหลังทำเสร็จ, low หรือ high puncture site)
- ผู้ป่วยเอง (อายุมาก, อ้วน, hypertension, peripheral artery disease)
Diagnosis
- Most common clinical presentation = pain, swelling in the groin after catheterization
- Physical exam: palpable pulsatile mass or systolic bruit
- Diagnostic examination of choice = color Doppler ultrasound
Ultrasound Findings
- Grey scale: anechoic sac (PSA) near the native artery (CFA) (ตามรูปด้านบน)
- Color Doppler: to-and-fro signal, tract connecting native vessel with PSA
สิ่งควรคำนึงเวลาทำอัลตราซาวด์
- ต้องหา native vessel ใกล้เคียงให้เจอและต้อง record flow ที่ตำแหน่ง proximal และ distal ต่อ PSA
- ขนาดของ PSA neck (tract เชื่อมระหว่าง native artery กับ PSA)
- วัดขนาดของ PSA
- Rule out DVT ที่อาจเกิด secondary to prolonged commpression on the groin or pressure from expanding hematoma
- ใช้ linear transducer
- ปรับความลึกให้เหมาะสม จะได้ไม่ miss PSA ที่อยู่ลึก
Reference: Webber, et al. Circulation 2007;115:2666-2674
April 19, 2008
Suspected Acute Appendicitis (3) - When and Why Doing Imaging Studies?


เป็นที่ทราบกันอยู่แล้วว่าทางเลือกหนึ่งในการวินิจฉัย acute appendicitis คือการทำ imaging study นะครับ บทบาทของ imaging study จะอยู่ที่การช่วย diagnosis, exclude acute appendicitis และการให้ alternative diagnosis
Clinical exam มีข้อจำกัด*
- Underdiagnosis: ประมาณ 20% rate of missed appendicitis
- Over diagnosis: 15%-40% false positive appendectomy
จะทำ ultrasound หรือ CT ในกรณีที่สงสัยว่าผู้ป่วยอาจเป็น acute appendicitis?
น่าจะทำ Ultrasound ถ้า
- ผู้ป่วยเป็นเด็ก (radiation exposure)
- ผู้ป่วยเป็นผู้หญิงวัยเจริญพันธุ์ (alternative gynecologic diagnosis, radiation exposure)
- ผู้ป่วยเป็นหญิงตั้งครรภ์ (radiation exposure)
- ผู้ป่วยผอม (easier to scan)
- รังสีแพทย์มีประสบการณ์ในการทำอัลตราซาวด์ appendix
น่าจะทำ CT ถ้า
- ผู้ป่วยอายุมาก (alternative diagnosis)
- ผู้ป่วยอ้วน
- อาการปวดท้องไม่ชัดเจนหรือปวดทั่วๆ (alternative diagnosis)
- มีความพร้อมด้านเครื่องมือและเทคนิกในการตรวจ appendiceal CT
เปรียบเทียบ Appendiceal ultrasound กับ CT
Ultrasound sensitivity 86%, specificity 81%**
CT sensitivity 94%, specificity 95%**
* N Engl J Med 1998;338:141
** Ann Intern Med 2004;141:537
Above images from GE Healthcare and Seimens Medical Solutions websites
April 15, 2008
Writing MCQs - Importance of Objectives

April 12, 2008
Corner of Radiograph
อย่าลืมมองที่มุมของภาพ (ไม่ว่าจะเป็นฟิล์ม หรือ digital image) ทุกครั้งว่ามี lesion หรือ clue อะไรที่จะนำเราไปสู่การวินิจฉัยโรค ภาพเอกซเรย์ข้างบนเป็นตัวอย่างของผู้ป่วยชายอายุ 33 ปีที่มาด้วยประวัติ trauma พบว่ามี osteochondral fracture ที่ talar dome (ลูกศรแดง) ซึ่งอยู่ที่ขอบภาพ ผู้ป่วยไม่มีอาการใดๆ มาก่อน ครั้งนี้เจ็บบริเวณกลางๆ ของขามากกว่า ทำให้ emergency medicine physician ส่งตรวจเอกซเรย์ leg แทนที่จะเป็น ankle
ภาพเอกซเรย์ข้างบนเป็นตัวอย่างของผู้ป่วยชายอายุ 33 ปีที่มาด้วยประวัติ trauma พบว่ามี osteochondral fracture ที่ talar dome (ลูกศรแดง) ซึ่งอยู่ที่ขอบภาพ ผู้ป่วยไม่มีอาการใดๆ มาก่อน ครั้งนี้เจ็บบริเวณกลางๆ ของขามากกว่า ทำให้ emergency medicine physician ส่งตรวจเอกซเรย์ leg แทนที่จะเป็น ankle ภาพซูมจากเอกซเรย์ ankle
ภาพซูมจากเอกซเรย์ ankle ภาพ MR (fat-suppressed PD coronal sequence) ทำเพื่อ stage Osteochondral injury. เราจะเห็นว่า lesion มีลักษณะเป็น bone fragment ที่แยกออกจาก talar dome ได้ด้วย fluid และ fragment นี้ไม่่ displaced จาก talar dome "Fluid around an undetached, undisplaced osteochondral fragment".
ภาพ MR (fat-suppressed PD coronal sequence) ทำเพื่อ stage Osteochondral injury. เราจะเห็นว่า lesion มีลักษณะเป็น bone fragment ที่แยกออกจาก talar dome ได้ด้วย fluid และ fragment นี้ไม่่ displaced จาก talar dome "Fluid around an undetached, undisplaced osteochondral fragment".
Facts:
- Common osteochondral injury (i.e. osteochondritis dissecans): Knee > Elbow, Ankle, Hip
- Talar osteochondral injury may occur at medial or lateral part of the talar dome
- Medial talar lesion commonly is asymptomatic, in contrast to lateral talar lesion
Reference: Schenck RC, Goodnight JM. Current concept review - osteochondritis dissecans. JBJS 1996; 78:439-456.
April 10, 2008
Flow analysis
การดู angiogram นั้น นอกจากการดูภาพในลักษณะของ 2D หรือ 3D แล้ว สิ่งสำคัญอีกอย่างหนึ่งคือการดู 4D คือ time
dimension วันนี้จะนำเสนอ trick เล็กๆน้อยๆเกี่ยวกับการดู dynamic จาก static study ครับ
บางคนคงบอกว่า ภาพ static จะบอกถึง dynamic ได้อย่างไร เราเริ่มดูจากรูปนี้กันก่อน

ทีนี้เราลองมาดูภาพ venogram ของแขนขวาในผู้ป่วยรายนี้กัน ผู้ป่วย ESRD มาด้วยแขนขวาบวมขึ้น
 สีฉีดผ่าน superficial vein แขนขวา จะเห็นได้ว่า สีวิ่งจาก 1 ไป 2 ไป 3 และย้อนลงมาตรงเบอร์ 4
สีฉีดผ่าน superficial vein แขนขวา จะเห็นได้ว่า สีวิ่งจาก 1 ไป 2 ไป 3 และย้อนลงมาตรงเบอร์ 4
น่าจะมี occlusion ตรง right axillary vein ใช่หรือเปล่าหนอ
เราลองสังเกตสิ่งที่น่าสนใจบางอย่างกันนะครับ
สีตรงเบอร์ 2 จางกว่าเบอร์ 1
สีตรงเบอร์ 3 จางกว่าเบอร์ 2
สีตรงเบอร์ 4 เข้มกว่าเบอร์ 2และ 3
ข้อเท็จจริงคือ เราฉีด contrast media ที่ความเข้มข้นเท่ากัน แต่เหตุใดหนอ สีจึงมีความเข้มข้นต่างกัน ลองคิดดูนะครับ
สีจางลงเพราะความเข้มข้นต่างกัน นั่นคือต้องมี เลือด จากที่ไหนเข้ามาเจือจางสีอย่างแน่นอน
ทีนี้ลองดูภาพเฉลยกันภาพนี้ฉีดสีผ่าน AVBG แขนซ้าย ทิศทางการไหลแสดงตามลูกศรสีขาว

จะเห็นได้ว่าแท้จริงแล้ว การที่เรามองไม่เห็น right axillary และ right subclavian veins นั้นเป็นเพราะว่ามี retrograde flow นั่นเอง และ retrograde flow นั้นก็เป็นตัวเจือจางสีดังที่เห็น
ลองหัดดูกับ angiogram อื่นๆดูนะครับ
April 9, 2008
Suspected Acute Appendicitis (2)


Left image: longitudinal scan shows a dilated fluid-filled tubular structure, measuring more than 6 mm in diameter.
Right image: transverse scan, without and with compression, shows noncompressibility of appendicitis.
Ultrasound
ข้อดี
1. วินิจฉัย appendicitis ได้ดีในคนผอม
2. วินิจฉัยภาวะอื่นทาง gynecology เช่น ovarian cyst, ectopic pregnancy
ข้อด้อย
1. ความแม่นยำขึ้นกับผู้ตรวจ
2. อาจไม่เห็น normal appendix ทำให้ไม่สามารถ exclude appendicitis ได้
2. วินิจฉัย complication ของ appendicitis ได้ไม่ดีเท่า CT
Ultrasound Findings of Acute Appendicitis
1. Enlarged dilated appendix, >/= 6 mm in cross-sectional diameter
2. Noncompressible appendix
3. Appendicolith(s)
4. (indirect) Phlegmon, fluid collection in right lower quadrant
'Visualization of NORMAL appendix rules out acute appendicitis'
สิ่งสำคัญที่ต้องคำนึงถึงในการตรวจผู้ป่วยสงสัยว่าเป็น acute appendicitis ด้วย ultrasound
1. ต้องใช้ graded compression technique
2. High-frequency tranducer (typically linear transducer)
3. อย่าลืมหา ovary ด้วย (ในผู้หญิง)
4. ถ้าไม่เห็น normal appendix ก็ยังไม่สามารถ exclude acute appendicitis ได้ แนวทางการตรวจต่อไปจะขึ้นกับ clinical findings อาจทำการ observe, re-exam with ultrasound, CT, หรืออาจผ่าตัด
5. CT น่าจะมีประโยชน์มากกว่าถ้าผู้ป่วยอ้วน, สูงอายุ (มีโอกาสเป็นโรคอื่นที่คล้าย appendicitis)
April 4, 2008
Suspected Acute Appendicitis (1)
โดยทั่วไปที่ร่ำเรียนกันมาผ่านศัลยกรรม อายุรกรรม หรือว่าเด็ก ก็คงรู้กันว่า appendicitis เป็น clinical diagnosis นะครับ ถามว่าเมืื่อสงสัยว่าคนไข้อาจเป็น acute appendicitis มีทางเลือกอะไรบ้าง
1. Observation
- ข้อดี คือ เพ่ิมความแม่นยำในการวินิจฉัยเนื่องจากอาการชัดเจนขึ้น
- ข้อเสีย คือ เพ่ิมความเสี่ยงในการเกิด ruptured appendicitis ซึ่งทำให้ morbidity และ mortality สูงขึ้นโดยเฉพาะในคนไข้เด็กและผู้สูงอายุ, เสียค่าใช้จ่ายจากการ admit คนไข้เข้าห้องสังเกตอาการ
2. Diagnostic imaging e.g ultrasound, CT
- ข้อดี คือ เพ่ิมความแม่นยำในการวินิจฉัย โดยการ exclude ภาวะอื่นที่อาจมีอาการคล้ายกันออกไป และ อาจวินิจฉัยภาวะ acute appendicitis ได้โดยตรงจากการตรวจ
- ข้อเสีย คือ test ทุกอย่างมีข้อจำกัด โดยที่ไม่มี test ไหนมี accuracy 100%, ค่าใช้จ่ายที่ใช้ในการตรวจ, เวลาในการรอตรวจ
3. Laparoscopy, Appendectomy
- ข้อดี คือ เป็นวิธีที่แน่นอนที่สุดในการวินิจฉัยภาวะนี้
- ข้อเสีย คือ ความเสี่ยงจากการดมยา การผ่าตัด (โดยเฉพาะในคนไข้ที่อาจไม่ได้เป็น acute appendicitis แต่ต้องไปเสี่ยงกับการผ่าตัดและดมยาโดยไม่จำเป็น) และค่าใช้จ่าย
หัวข้อถัดไปจะพูดถึงในแง่ของ Diagnostic Imaging สำหรับการวินิจฉัยภาวะนี้ครับ
Pros and Cons of Ways to Diagnose Acute Appendicitis:
1. Observation: get more accuracy from clinical examination but will risk having perforated appendicitis
2. Diagnostic imaging: more accuracy than getting data from clinical exam alone but will cost more and the tests have certain accuracy (not 100%)
3. Laparoscopy, appendectomy: best way to diagnose this but may result in negative appendectomy (unnecessary anesthesia, and surgery)
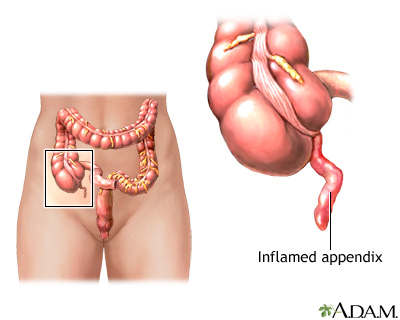
Above image from: MedlinePlus
April 2, 2008
Evaluate level of lung inflation in pediatric chest film

หลายคนคงเคยประสบปัญหาว่าทำไมฟิล์มเอกซเรย์ในเด็กแปลผลได้ยาก
 ส่วนหนึ่งเกิดจากการอ่านฟิล์มที่ inadequate inspiration นั่นเอง แล้วเราจะทราบได้อย่างไรว่าฟิล์มนี้ adequate inspiration หรือไม่ หรือ เป็นฟิล์มในช่วง expiration มีหลักง่ายๆมาฝากค่ะ
ส่วนหนึ่งเกิดจากการอ่านฟิล์มที่ inadequate inspiration นั่นเอง แล้วเราจะทราบได้อย่างไรว่าฟิล์มนี้ adequate inspiration หรือไม่ หรือ เป็นฟิล์มในช่วง expiration มีหลักง่ายๆมาฝากค่ะการประเมินระดับการหายใจในเด็กต้องใช้หลายอย่างประกอบกันได้แก่
1. การนับกระดูกซี่โครงเทียบกับ dome of diaphragm ในเด็กนิยมใช้ anterior rib มากกว่า posterior rib เนื่องจากยอดของกะบังลมในเด็กส่วนมากอยู่ด้านหน้า ฟิล์มเอกซเรย์ปอดที่ adequate inspiration จะพบขอบของกะบังลมอยู่ในระดับ 6th anterior rib หรือ 9th posterior rib หากขอบของกะบังลมอยู่ต่ำกว่า 8th anterior rib หรือ 10th posterior rib แสดงว่า hyperaeration หรือมีภาวะ air
 trapping
trapping
2. ลักษณะรูปร่างของกะบังลมซึ่งสังเกตได้ทั้งจากท่า AP และ lateral view
หากกะบังลมมีลักษณะแบน (flattening) แสดงว่ามีภาวะ hyperaeration
3. ขอบเขตด้านล่างของหัวใจเมื่อเทียบกับขอบของกะบังลม หากขอบของหัวใจทั้งหมดอยู่เหนือกะบังลมแสดงว่า hyperaeration หากขอบของหัวใจด้านล่างอยู่ใต้ขอบของกะบังลมมาก
แ สดงว่าหายใจเข้าไม่เต็มที่
4. ลักษณะโค้งงอของหลอดลม หรือ tracheal buckling ซึ่งจะพบได้ในฟิล์ม expiration
จากรูปด้านบน (รูปที่ 1) จะพบว่าเป็น expiration film ซึ่งสังเกตได้จากลักษณะ tracheal buckling ขอบบนของกะบังลมอยู่ในระดับ 5th anterior rib และ 8th posterior rib และขอบล่าง
ของหัวใจอยู่ใต้ขอบกะบังลมมาก
รูปที่ 2 แสดงให้เห็นว่าเราอาจแปลผลฟิล์มว่ามี patchy opacity ที่ right lung แต่เมื่อเราประเมินแล้วเป็น film ที่ inadequate inspiration จึงได้นำผู้ป่วยไปถ่ายเอกซเรย์ใหม่ (รูปที่ 3)จะพบว่า abnormal opacity ได้หายไป
การประเมินระดับการหายใจนอกจากจะช่วยในการแปลผล chest film แล้วยังสามารถช่วยในการ diagnosis โรคได้อีกด้วยเช่น hypoaeration พบใน respiratory distress syndrome(RDS) หรือ pulmonary hypoplasia ซึ่งต่างจากภาวะอื่นได้แก่ retained fetal lung fluid, meconium aspiration syndrome (MAC) และ neonatal pneumonia จะพบลักษณะ hyperaeration
April 1, 2008
Pneumothorax Versus Skin Fold
 ดูเหมือนจะแยกจากกันไม่ยากใช่มั้ยครับ ระหว่าง skin fold กับ visceral pleural line of pneumothorax โดยมากก็จริงว่าแยกกันไม่ยากครับ แต่บางครั้งก็สร้างปัญหาได้เหมือนกันครับ วันนี้ได้เอาภาพมาให้ดูเทียบกันชัดๆ เพราะทั้ง 2 ตัวอย่างอยู่ในภาพเดียวกัน แถมยังข้างขวาเหมือนกันซะด้วยครับ
ดูเหมือนจะแยกจากกันไม่ยากใช่มั้ยครับ ระหว่าง skin fold กับ visceral pleural line of pneumothorax โดยมากก็จริงว่าแยกกันไม่ยากครับ แต่บางครั้งก็สร้างปัญหาได้เหมือนกันครับ วันนี้ได้เอาภาพมาให้ดูเทียบกันชัดๆ เพราะทั้ง 2 ตัวอย่างอยู่ในภาพเดียวกัน แถมยังข้างขวาเหมือนกันซะด้วยครับ
ในภาพนี้จะเห็นว่า visceral pleural line of pneumothorax (ลูกศรสีแดง) ขอบชัด ใช้ดินสอขีดได้ (ภาษาพูดจะบอกว่าเป็น Line) ขอบนอกกว่า pneumothorax ก็จะไม่มี lung markings แต่ skin fold (ลูกศรสีเขียว) จะเป็นแถบที่หนากว่า (band, edge) ไม่ใช่ เส้น (Line) ร่วมกับมี radiolucent band ฉาบอยู่ด้านนอกซึ่งเรียกว่า Mach Band และส่วนใหญ่เราจะเห็นว่า skin fold ยื่นออกไปนอกตัวปอดด้วยครับ
จะทำยังไงถ้าแยกกันไม่ออก มีคำแนะนำครับ
1. ทำเอกซเรย์เพิ่ม เช่น decubitus view, end-expiratory view
2. follow up x-ray ด้วย PA upright view
3. แต่ถ้าอาการคนไข้ไม่คงที่ ก็ต้องรักษาไปตามอาการนะครับ ไม่ใช่มัวแต่เอกซเรย์กันอยู่
Pneumothorax: sharp line, not extend beyond rib cage, no lung markings beyond the line
Skin fold: edge/band (not line), extend beyond rib cage, Mach Band noted periphery to it, lung markings present beyond the edge
Reference: AJR Am J Roentgenol. 1978 Apr;130(4):791-2.
What is this ocular prosthesis called?



Scleral buckle or scleral buckling device.
It is a device designed to treat retinal detachment. Retinal detachment is a disease when there is a separation of the sensory retina from the underlying pigment epithelium. The device indent the sclera and keep the retinal layers adheres to each other.
The device can be placed encircling the globe or radially (parallel to the axis of the extraocular muscles). It can complete 360 degree around the globe or segmentally.
The device is made of silicone. There are 2 main components: outer solid silicone rubber (hyperdense on CT) and inner silicone sponge (air density on CT). Both are hypointense on T1 and T2WI and radiolucent on plain radiographs).
This patient has a scleral buckle encircling around his left eye after suffering from a retinal detachment. Uniquely, there is only hyperdense silicone rubber band, without silicone sponge.
What does the clinician want to know? The clinician would like us to mention the integrity of the device, sign of infection and the presence or absence of choroidal detachment which is the most common complication after the procedure.
Reference: Retinal Detachment: Imaging of Surgical Treatments and Complications. Radiographics 2003;23:983-994












