|
| (A) MIP image from a PET/CT shows areas of FDG avidity in multiple lymph node stations including hilar, mediastinal, axillary, upper abdominal and groin regions. Note intense uptake of the spleen. |

 |
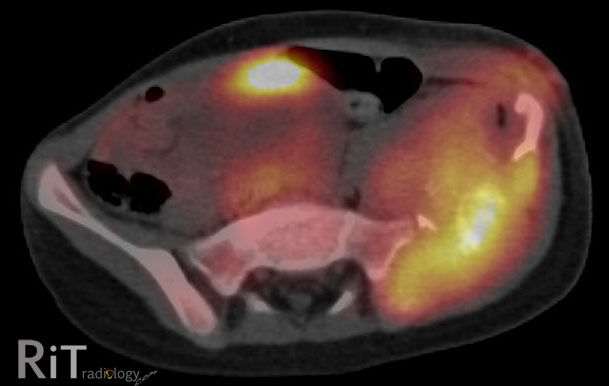
| (B&C) Axial fused PET/CT images show intense FDG uptake within thoracic, axillary nodes and spleen. |
PET/CT: Three patterns of sarcoidosis
- Typical: Bilateral hilar uptake extending to the mediastinum with bilateral lung uptakes (PET and CT concordant lesions). This is found in the majority of cases (about 2/3)
- Discrepant: Multiple foci of uptake in and outside chest, along with splenic uptake (PET and CT discordant lesions). Fewer lesions are seen on CT than on PET. This pattern is the 2nd most common and is indistinguishable from malignancy (esp. metastasis, lymphoma)
- Multiple small FDG avid lung lesions: This pattern is similar to lung metastasis. Fortunately, it is the least common pattern.
Our case: Biopsy-confirmed sarcoidosis involving the hilar, mediastinal, upper abdominal lymph nodes, and spleen. This follows the "discrepant" pattern (basically meaning that malignancy cannot be reliably distinguished)
References:
Alavi A, et al. Positron emission tomography imaging in nonmalignant thoracic disorders. Semin Nucl Med 2002;32:293-321.