Author: พ.ญ. นิธิมา ศักดิ์โสภาวิวัฒน์ คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี
Editor: น.พ. รัฐชัย แก้วลาย คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี
ประวัติ:
ผู้ป่วยชาย อายุ 27 ปีมาตรวจที่แผนกฉุกเฉินด้วยอาการเจ็บคอด้านขวา
ร่วมกับอาการกลืนเจ็บ กลืนลำบาก เป็นมาประมาณ 10 วัน ต่อมามีไข้ และหายใจลำบาก
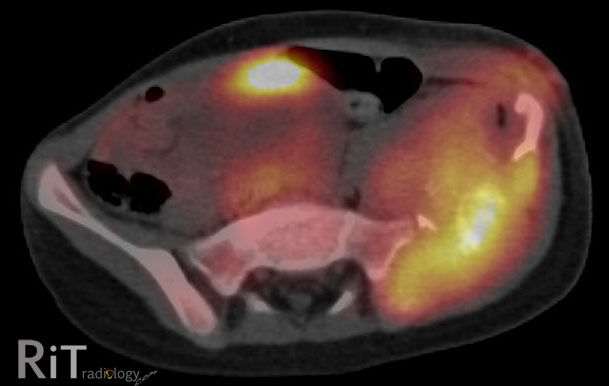
ภาพที่ 1 เป็น axial CT ส่วนคอแสดงให้เห็น rim-enhancing fluid
collection ทางด้านขวา หน้าต่อ carotid space. ภายใน carotid space ไม่เห็น
internal jugular vein ที่ปกติ แต่ถูกแทนที่ด้วย hypodense filling defect ร่วมกับผนังของหลอดเลือดดำมี
enhancement. ภาพที่ 2 เป็นภาพ coronal
reformation เพ่ิมเติม แสดงให้เห็น filling defect ภายใน internal jugular vein ข้างขวาและ
enhancement ของผนังหลอดเลือดนี้. ภาพที่
3 เป็นภาพ axial CT ทรวงอกใน lung window แสดงให้เห็น pulmonary nodules ขนาดเล็กกว่าหนึ่งเซนติเมตรในปอดทั้งสองข้าง
บางอันมี cavity ภายใน สังเกตว่า nodules มักอยู่ที่รอบนอกของปอด (Image courtesy
of University of Maryland Medical Center, MD, USA)
การวินิจฉัยโรค Lemierre
Syndrome
Discussion ผู้ป่วยรายนี้มาพบแพทย์เนื่องจากมีการอักเสบติดเชื้อที่ต่อมทอนซิลและเกิด
peritonsillar abscess ทำให้มี thrombophlebitis ของ internal jugular vein ที่อยู่ติดกันและมี
septic emboli กระจายไปยังปอดทั้งสองข้าง
โรคติดเชื้อในช่องปากและคอที่มีภาวะแทรกซ้อนเช่นนี้รู้จักกันในชื่อ
Lemierre syndrome ซึ่งตั้งตามชื่อแพทย์ผู้รายงานกรณีผู้ป่วย 20 ราย ในปี พ.ศ. 2479
(1) ในปัจจุบันพบโรคนี้น้อยมากเนื่องจากมีการใช้ยาปฏิชีวนะกันอย่างแพร่หลาย
แต่การวินิจฉัยภาวะนี้ให้รวดเร็ว แม่นยำ ยังมีความสำคัญเพราะหากได้รับการรักษาช้าอาจทำให้เสียชีวิตได้
Lemierre syndrome ส่วนใหญ่เกิดจากการติดเชื้อ
anaerobic Fusobacterium necrophorum เมื่อมีการติดเชื้อที่ช่องคอ
ทอนซิลหรือช่องปากแล้วอาจมีการแพร่กระจายโดยตรง, ผ่านทางหลอดเลือดรอบๆต่อมทอนซิลหรือผ่านทางท่อน้ำเหลืองไปยัง
internal jugular vein ทำให้เกิด thrombophlebitis และ septic emboli กระจายไปยังอวัยวะอื่นๆ
ได้ ที่พบบ่อยที่สุดคือปอด
(79-100%) ผู้ป่วยส่วนมากเป็นวัยรุ่นแต่ก็พบได้ทุกอายุ มักมาพบแพทย์ด้วยอาการเจ็บคอ
มีไข้ บวมกดเจ็บ และอาการอื่นๆ ขึ้นกับตำแหน่งการแพร่กระจายของ septic emboli (2, 3).
การตรวจทาง imaging
มีบทบาทมากในการวินิจฉัยภาวะนี้ อัลตราซาวด์สามารถแสดงให้เห็นลิ่มเลือดที่อยู่ภายใน
internal jugular vein ได้ดี ไม่ว่าจะเป็นชนิดที่มีการอุดกั้นหรือไม่ก็ตาม หรืออาจเห็นลักษณะ
venous distension, absent flow หรือ non-compressible vein. การตรวจด้วย CT ร่วมกับการให้สารทึบรังสีชนิดฉีดจะแสดงขอบเขตของการติดเชื้อ
เช่น peritonsillar abscess ได้ดีกว่าอัลตราซาวด์ และแสดงภาพลิ่มเลือดเป็น filling
defect ภายในหลอดเลือดดำ หลอดเลือดดำดังกล่าวอาจมีขนาดใหญ่ขึ้นร่วมกับมี
fat stranding รอบๆ และมี enhancement ของผนังหลอดเลือด. การตรวจเอกซเรย์ปอดอาจพบว่ามี
pulmonary nodules, masses, cavitary lesions, focal airspace disease ได้แต่การทำเอกซเรย์คอมพิวเตอร์จะให้รายละเอียดได้ดีกว่า
ความผิดปกติที่พบในปอดมักอยู่ที่บริเวณรอบนอก (periphery) ของเนื้อปอด เข้าได้กับ
septic emboli หากสงสัยภาวะนี้ ผู้ป่วยควรได้รับการตรวจ
CT ของทรวงอกและคอในคราวเดียวกัน การรักษาได้แก่การให้ยาปฏิชีวนะ
ยาละลายลิ่มเลือด และการผ่าตัด (4).
เอกสารอ้างอิง
1. Lemierre
A. On certain septicemias due to anaerobic organisms. Lancet 1936; 1:701-703.
2. Karkos
PD, Asrani S, Karkos CD, et al. Lemierre's syndrome: A systematic review.
Laryngoscope 2009; 119:1552-1559.
3. Vargiami
EG, Farmaki E, Tasiopoulou D, et al. The Lemierre syndrome. Eur J Pediatr 2010;
169:411-414.
4. Weeks
DF, Katz DS, Saxon P, Kubal WS. Lemierre syndrome: report of five new cases and
literature review. Emerg Radiol 2010; 17:323-328.