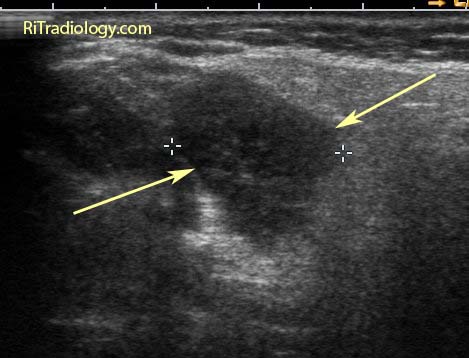
A longitudinal ultrasound image of the kidney shows a focal depression of the lower pole cortex (arrows) with focal parenchymal thinning and a caliceal stone (between calipers).
Facts:
- Renal scar is a common incidental finding during imaging of the GU tract
- It can occur both with and without episodes of infundibular obstruction
- Reflux is considered a major contributor in development of non-obstructive scarring, particularly in children with vesicoureteric reflux (VUR)
- In adults, renal scarring is more associated with renal stone disease, either with stone or history of stone
Imaging
- Focal cortical thinning and depression of the cortex, overlying the pyramid on any imaging modalities (IVU, US, CT, MR)
- Hyperechoic band is seen over the parenchymal thinning on US
- Mimic = normal renal lobulation. Lobulation will span the pyramids with echogenic lobular junctions into renal columns
Reference:
Newhouse JH, Amis, Jr, ES. The relationship between renal scarring and stone disease. AJR 1988; 151:1153-1156.